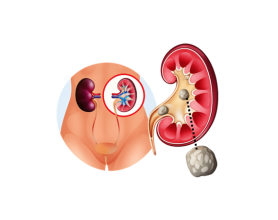
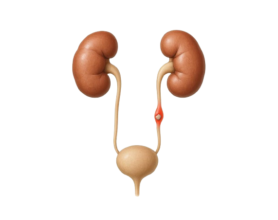
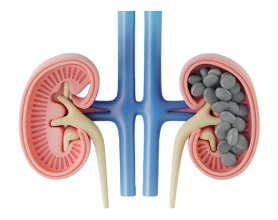
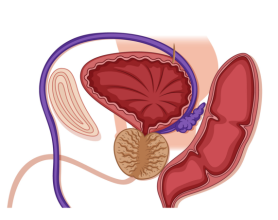
About Pelvi‑Ureteric Junction (PUJ) Obstruction
Pelvi‑Ureteric Junction (PUJ) obstruction arises when the connection between the renal pelvis (the kidney’s urine‑collecting chamber) and the ureter becomes narrowed or blocked, impeding urine flow from the kidney. Congenital forms affect roughly 1 in 500–1,000 live births, while acquired causes like stones or trauma vary. If untreated, PUJ obstruction can result in progressive kidney damage, hypertension, or even renal failure.
Signs and Symptoms of PUJ Obstruction
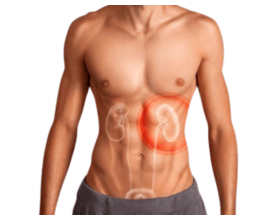
1. Flank Pain
- Description: Dull, persistent ache or sharp, colicky pain in the side or back typically between ribs and hip on the affected side.
- Cause: Urine backup stretches the renal capsule or raises intrapelvic pressure, activating nerve endings. Intermittent obstruction may mimic classic kidney stone pain.
- Triggers: Symptoms may worsen after fluid intake,such as water, alcohol, or large meals—because elevated urine output increases pressure at the obstruction; alcohol’s diuretic action can magnify discomfort.
- Patterns: Chronic cases often present with constant dull ache; acute episodes are more episodic and sharp, sometimes radiating toward lower abdomen or groin.
- Intensity: Ranges from mild discomfort to debilitating pain, depending on the severity of obstruction and kidney response.
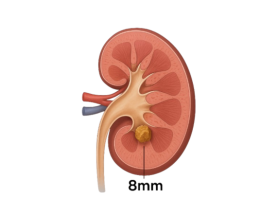
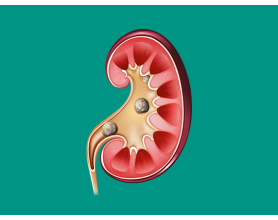
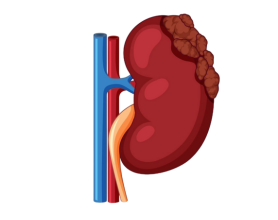
2. Hydronephrosis
- Description: Swelling of the kidney caused by urine accumulation in the renal pelvis and calyces, blocked at the PUJ.
- Cause: Obstruction creates a “traffic jam,” causing back‑pressure into the kidney; congenital cases are often seen prenatally, whereas acquired ones develop gradually.
- Symptoms: Many mild or moderate cases remain asymptomatic initially; severe hydronephrosis can cause flank pain, a palpable mass (especially in lean adults or children), or a sensation of fullness.
- Progression: Ongoing swelling can thin the renal parenchyma, increasing the risk of irreversible damage.
- Detection: Often identified by ultrasound or CT before symptoms manifest—these imaging findings are crucial for diagnosis.
3. Recurrent Urinary Tract Infections (UTIs)
- Description: Frequent UTIs, particularly involving the kidney (pyelonephritis).
- Cause: Stagnant urine above the PUJ provides a breeding ground for bacteria, compounded by poor drainage. Partial obstruction increases susceptibility.
- Symptoms: Fever, chills, dysuria, cloudy or smelly urine, flank pain if the kidney is involved. Recurrent UTIs warrant investigation for underlying obstruction.
- Risks: Especially prevalent in children with congenital PUJ obstruction or adults with stones or scar tissue.
- Complications: Untreated infections may cause renal scarring or systemic spread like sepsis.
4. Nausea & Vomiting
- Description: Nausea or vomiting frequently accompanies flank pain or significant renal impairment.
- Cause: Acute pain can activate the vagal response, eliciting nausea. Hydronephrosis‑related pressure or accumulation of uremic toxins may contribute in advanced cases.
- Context: More common during acute pain episodes particularly after fluid loading or in children with marked obstruction.
- Severity: Can range from mild queasiness to recurrent vomiting, especially if pain is episodic or infection coexists.
- Association: Usually secondary but distressing, and closely tied to pain episodes.
5. Hematuria (Blood in Urine)
- Description: Gross (visible) or microscopic blood in the urine, altering its color to pink, red, or brown.
- Cause: Irritation or micro‑trauma at the PUJ most often from stones scraping the mucosa—or stretching of the renal pelvis may rupture small vessels. Chronic congenital narrowing can also result in microscopic bleeding.
- Presentation: Gross hematuria is noticeable and typically linked to stones or trauma; microscopic hematuria is often incidental.
- Significance: Any hematuria calls for evaluation to exclude stones, tumors, or significant obstruction.
- Frequency: Often intermittent may coincide with activity, hydration changes, or stone movement.
6. Reduced Urine Flow
- Description: Lower urine volume or sluggish stream not as obvious as lower tract causes, but possible in high‑grade or bilateral obstruction.
- Cause: Significant blockage limits urine passage to the bladder. Complete obstruction is rare; partial cases often feature very slow drainage. Bilateral cases can markedly reduce output.
- Symptoms: Patients might notice reduced urine volume, hesitancy, or incomplete voiding but these signs may be overshadowed by pain or infection.
- Detection: More readily apparent during diagnostic tests (e.g., renal scintigraphy showing delayed drainage) than in daily life unless advanced.
- Implication: Suggests worsening obstruction or renal strain.
Symptoms In Children:
- Abdominal Mass: Hydronephrosis may present as a palpable abdominal lump especially in neonates or slender infants often noticed by parents or healthcare providers.
- Failure to Thrive: Chronic obstruction, infections, or vomiting can impair growth and weight gain.
- Vomiting: Frequent spit‑ups or vomiting in infants often due to obstruction‑related pressure or pain rather than gastritis.
- Prenatal Detection: Routine fetal ultrasounds frequently identify hydronephrosis, leading to postnatal diagnostic work‑up (e.g., MAG3 renogram) to confirm PUJ obstruction.
- Presentation: Symptoms may be subtle (irritability, low‑grade fever) or nonexistent until complications arise making early imaging vital.
Causes of PUJ Obstruction
- Congenital Narrowing (most common): Malformation at the PUJ present from birth.
- Crossing Vessels: An aberrant artery or vein compressing the PUJ and impeding flow.
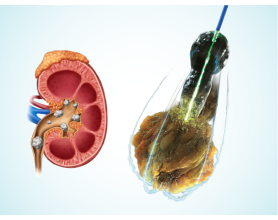
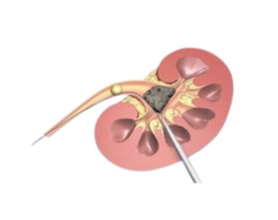
- Kidney Stones: Stones lodged near the PUJ can cause direct blockage, inflammation, and eventual scarring.
- Infection or Inflammation: Recurrent UTIs or pyelonephritis can lead to fibrotic narrowing.
- Post‑Surgical Scarring: Scarring following renal, ureteral, or retroperitoneal surgery.
- Tuberculosis or Chronic UTIs: Long‑standing infections may cause fibrosis and obstruction.
- Tumors or Extrinsic Compression: Rare cases where masses outside the urinary tract compress the PUJ.
These causes often culminate in hydronephrosis and, if unaddressed, progressive renal impairment.
Risk Factors of PUJ Obstruction
- Family History: A genetic predisposition exists—congenital PUJ obstruction may occur more in families, sometimes alongside other urinary malformations (e.g., duplex systems, VUR). If a first‑degree relative is affected, early postnatal screening is warranted.
- Age:
- Congenital cases: Typically detected in infancy via prenatal or neonatal imaging, though some remain silent until adulthood.
- Acquired cases: More common with increasing age due to accumulated insults—like stones, trauma, or prior surgery.
- Kidney Stones: Recurrent stone formers are at elevated risk for acquired PUJ obstruction; in addition, preexisting obstruction can lead to stone formation (creating a vicious cycle).
- Gender: Congenital PUJ obstruction shows a male predominance (~2:1). In adults, gender differences blur, although men have higher stone risk and women may face surgical scarring (e.g., post‑hysterectomy).
- Previous Surgery: Urological or retroperitoneal procedures near the kidney or ureter raise the risk of scarring and PUJ involvement.
Complications for PUJ Obstruction
- Chronic Kidney Damage: Prolonged hydronephrosis compresses the renal cortex and medulla, reducing filtration. Early treatment like pyeloplasty can preserve function, but delays may lead to irreversible atrophy or chronic kidney disease.
- Recurrent or Severe Infections: Stagnant urine invites bacteria to multiply, leading to pyelonephritis, abscess, or sepsis. Recurrent episodes can scar the kidney.
- Stone Formation: Concentration of minerals in stagnant urine favors crystallization. Stones can worsen obstruction and provoke pain or hematuria perpetuating a cycle.
- Hypertension: Obstructive stress activates the renin–angiotensin system, often causing elevated blood pressure more common in bilateral or severe cases, particularly in children.
- Renal Failure (Rare): Bilateral or advanced unilateral obstruction may result in reduced overall kidney function; in extreme cases, renal failure requiring dialysis or transplant may develop.
- Chronic Pain: Persistent or recurrent flank pain can impair quality of life. While relief often follows correction of obstruction, residual discomfort may persist.
Diagnosis of PUJ Obstruction
- Ultrasound: First‑line tool reveals hydronephrosis without ureteral dilation distal to the PUJ.
- CT Scan (Non‑contrast or Contrast-Enhanced): Offers detailed anatomy, detects stones, and excludes masses.
- MAG3 Renal Scintigraphy: Evaluates renal drainage; prolonged tracer retention (e.g., >20 minutes) suggests obstruction.
- Intravenous Pyelogram (IVP): Traditional radiographic study with dye to visualize urinary tract less common now due to CT.
- Ureteroscopy: When imaging is unclear, direct endoscopic inspection may be warranted.
- Prenatal Screening: Hydronephrosis detected in utero prompts post‑natal follow‑up (imaging + functional studies).
PUJ Obstruction Treatment
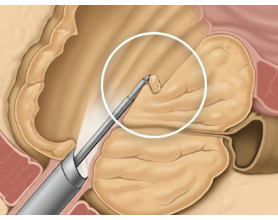
Definitive Repair – Pyeloplasty
Minimally invasive techniques like 3D laparoscopic pyeloplasty offer high precision and faster recovery by reconstructing and widening the PUJ with a three‑dimensional visual field, improving surgical outcomes.
Symptom & Risk‑Based Management
- Pain Relief: NSAIDs or other analgesics under physician direction.
- Infection Control: Prompt antibiotics for UTIs or pyelonephritis.
- Stones: If stones contribute, treatments like lithotripsy or ureteroscopy may be necessary alongside PUJ repair.
All treatments must follow licensed medical guidance.














































































 Explore More
Explore More